

On Oct 26, the government announced that the conditional movement control order (MCO) in Selangor and Federal Territories of Kuala Lumpur and Putrajaya would be extended for another two weeks, citing the current development of Covid-19 infection in the Klang Valley as the reason.
The conditional MCO would also now be implemented in Nilai, Negeri Sembilan from Oct 28 to Nov 10 following the surge of positive cases among foreigners in the area.
The imposition of the conditional MCO two weeks ago already stirred grouses amongst the public who are now facing the prospect of further extensions. When the extension was announced yesterday, Malaysia recorded 1,240 new Covid-19 cases and 9,744 active cases, of which 177 new cases were from Selangor, 17 in Kuala Lumpur and none in Putrajaya.
Before that, a disclaimer - this article is not to question whether the conditional MCO is justifiable or not. Instead, it is a reflection on how our leadership, health policymakers and other stakeholders can collectively best use these extra two weeks that are given by the people. After all, we must make sure their sacrifices are worthwhile this time.
To examine the situation, we shall begin with facts and data that we know.
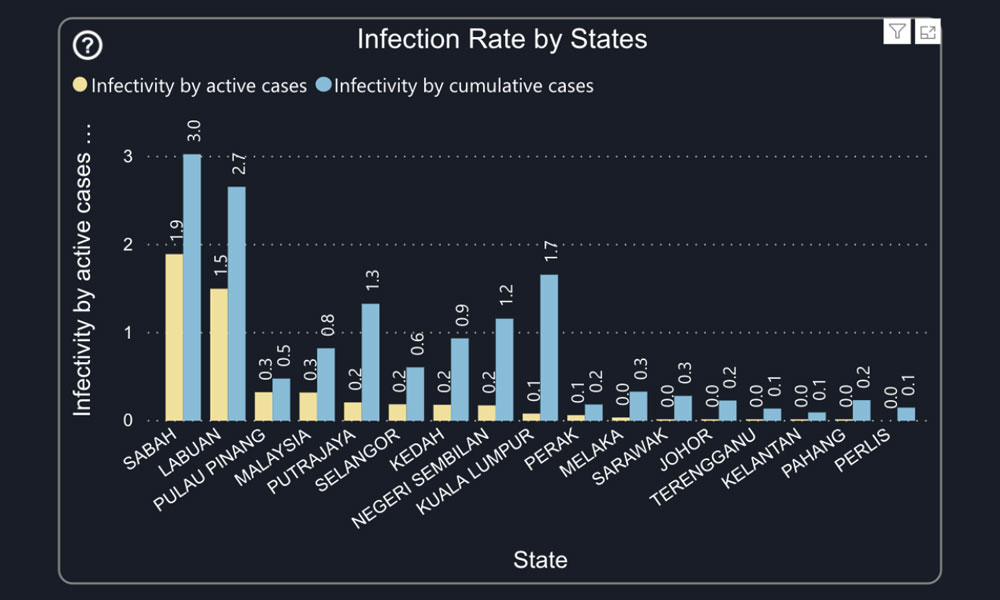
Average infectivity rate per population
The first point to consider is the Covid-19 average infectivity rate per population. In this article, we use an average infectivity rate per 10,000 population (i.e. current number of active cases / 10,000 population).
Seeing a daily increase in the number of new and active cases reported on the news is no doubt alarming. But the context is lost if one were to interpret the case number like a scoreboard. As we know, the reported case number is presented as is and not segregated according to population density.
Thus, it is inevitable that a densely populated area, such as Klang Valley that has more than seven million residents, will record a much higher number of Covid-19 cases, compared to a more sparsely populated state, for example, Negeri Sembilan.
Direct comparison of the number of cases, for instance, between Klang Valley with that of Negeri Sembilan, will not present an accurate infection picture of Covid-19. But the infectivity rate per population will present the number of Covid-19 cases recorded from various states in Malaysia in a comparable form.
Even so, the average infectivity rate still does not present us with the whole picture. To deploy an effective containment measure, the number of Covid-19 cases must also be considered according to the circumstances the virus was found. Cases found in a cluster require different containment measures than sporadic cases.
It is distorting to assume that all Covid-19 cases in Klang Valley carry a similar infectivity rate. A positive case in a prison (an isolated institution) would bring about different implications compared to a positive case detected within the community, via a random influenza-Like Illness (ILI) surveillance (this is when a patient with flu-like symptoms is chosen at random to undergo a Covid-19 test in a Klinik Kesihatan).
This brings us to our second point, clusters.
Clusters
Looking at a cluster gives us some advantage. This is because epidemiological links have already been established, and despite the growing number of cases (which will be, as a direct resultant of Contact Tracing), we can at least be certain that it is a “known” phenomena.
However, some clusters raise more concerns than others.
As an example, whilst it is unfortunate that Covid-19 found its way and formed clusters in detention centres, these clusters are highly isolated from the community and thus pose less risk for community transmission.
On the other hand, clusters found in the community (for e.g. those that originated from workplace, event-based or family) is more of a concern. Such a cluster can spread to individuals beyond the case index social circle.
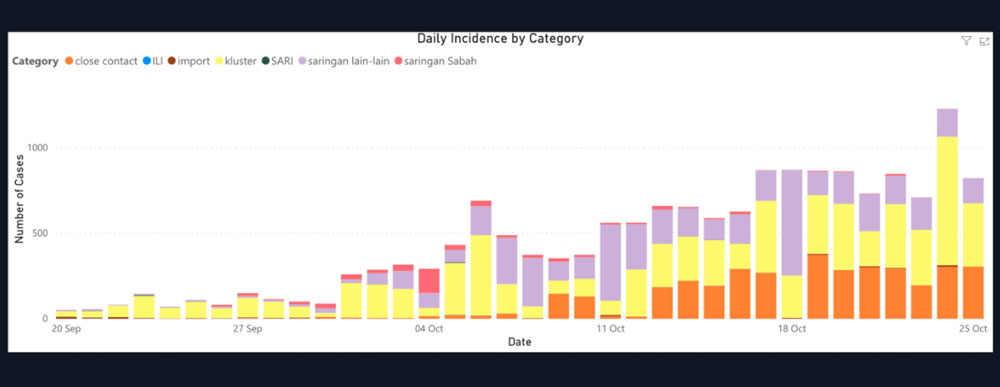
Currently, there are 44 clusters that are still active in the Klang Valley, and alarmingly, the major proportion of them are “Clusters in Community”.
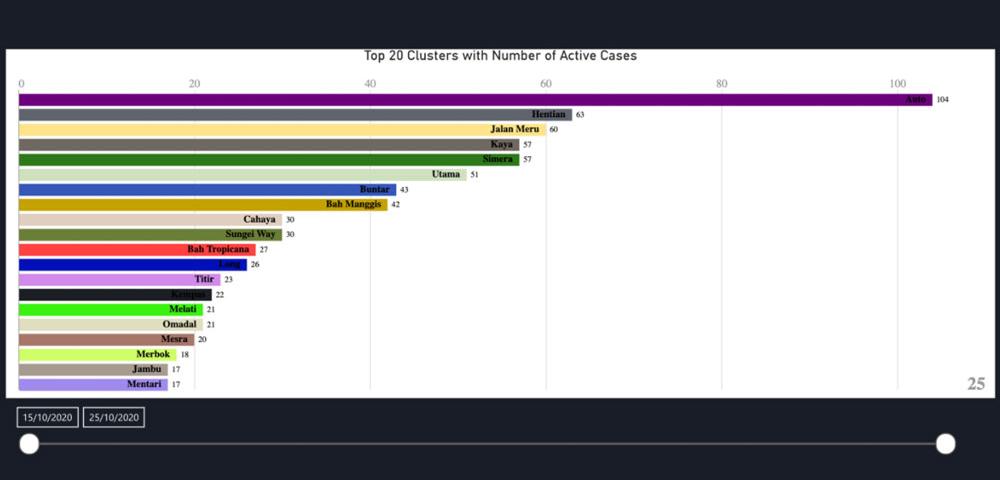
We can, however, take consolation that after the clusters’ initial identification, most of the “clusters in community” in Klang Valley does not grow dramatically in terms of its size.
Sporadic Cases
Whilst less popular and without a fancy name assigned to it (unlike, for example, Bah Tropicana cluster), sporadic cases are the more concerning parameter when we talk about “community transmission”. This is because they represent cases in a community that is randomly found - the more random cases are found, the more prevalent the infection is in the community.
Sporadic cases also present more challenges for healthcare workers. More sporadic cases mean more investigation needs to be done, more contact tracing to be conducted, more swab testing, and undoubtedly all these require more manpower.
So, how does the percentage of sporadic cases vs clusters in the Klang Valley look like?
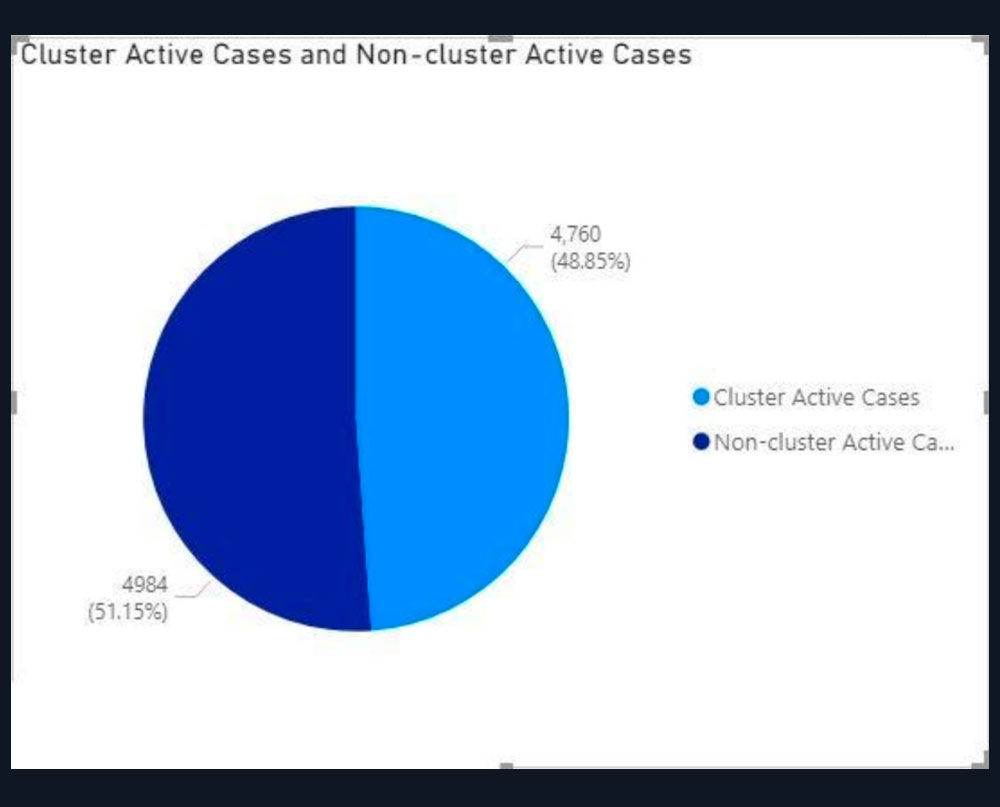
Unsatisfactory. Over the last seven days, the proportion of sporadic cases has increased to 51.15 percent. This means there are 4,984 individual cases that are not part of any cluster, hence requiring its own set of epidemiological investigation, contact tracing list, and human personnel to conduct all that.
Of course, once investigations and contact tracings are completed, any of these sporadic cases could potentially be traced to as a cluster and subsequently be reclassified into the “cluster categories”.
So is the conditional MCO extension justified?
If the rationale is to give more time for healthcare workers to catch up with investigations of all sporadic cases and at the same time to reduce risk of community transmission – the answer is yes, it is justified – with some pre-conditions (see below).
But if the rationale is to reduce community transmission to a single digit, this might be untenable with the current strategy.
We can see that for the past two weeks since the conditional MCO was implemented, the number of sporadic cases continued to increase.
With no other data point to rely on (for e.g. location of sporadic cases), the author had to assume the extension of the current measure of conditional MCO (i.e. closing some sectors state-wide, while opening others) would more or less produce the same effect.
Containment vs mitigation
If what we aim for is “containment” (i.e. to revert to the situation before Sept 27 and bring down the case number to a single digit), then the current conditional MCO measures are insufficient.
To achieve “containment” requires a stricter lockdown measure of a targeted area where sporadic cases are happening (e.g. a residential area or a condominium).
Without precise location data of sporadic cases, this is harder to be enacted. Sometimes, we are lucky if the residents are proactive and are aware of the emergence of multiple cases in their neighbourhood – for e.g. the Desa Puteri event and their resident task force initiative. Nonetheless, it should never be the residents’ job in the first place, especially when centralised data lies with the authorities.
A containment will also require a significant boost of public health resources to do contact tracing for all active cases in a detailed and timely manner. And we are not talking just about the number of hospital beds nor testing kits availability.
Covid-19 is an infectious disease that grows exponentially. Based on the Health Ministry’s (MOH) latest announcement, the national RT now is at 1.2, which means that each of 4,984 sporadic active cases shown in the pie chart above could infect another 1.2 people.
In containment - it really is a race against time to conduct TTI (trace, test, isolate) timeously. Do we have enough personnel (health inspectors) to sprint against it? Some countries hire up thousands of additional personnel (strategically, from all the industries that were affected by the lockdown) just to do contact tracing. Malaysia should invest in the same if we aim for containment.
If we fail to outrace the virus progression in its track – and we are quite likely to fail, given the limited resource we have to conduct contact tracing and based on the previous pattern of increasing sporadic cases – then we can only expect the case numbers to go up.
And it is unfortunate that going by the current logic, case numbers trending up is a good enough justification to prolong this lockdown.
Mitigation
Otherwise, we can be happy with “mitigation”, i.e. to accept that the virus is and will continue circulating in the community, and resign to the fact that we are going to live with it for a long time.
If we are content to opt for mitigation, we need to first “change our expectation”. As “containment” is no longer the objective, we should no longer colour code our zones using an arbitrary measure of green zones with zero cases, yellow as one to 40 cases and red as having more than 40 cases.
We must find a baseline of prevalence in the said community, so we can better titrate our “alert threshold”.
For all we know, if for example, the prevalence of Covid19 is 1.0 percent in Klang Valley, an area with seven million people, hence hypothetically 70,000 cases are present in the community at any given time.

Hence to lock down an area just because it registers more than 40 cases is overkill. The threshold for red, yellow, and green zones in Klang Valley then needs to be adjusted accordingly.
Even using the above example of a hypothetical 70,00 cases, this does not mean that we have to abandon these cases and just let the virus spread without taking any action. We still have to continue to identify, test, isolate, and treat. This exercise should be repeated until a vaccine is found. In fact, more repetitive than one thought it will be as Covid-19 survivors are not immune to another infection.
But at least we would not have to race against time during a lockdown period to attempt to reduce case number to a single digit. We accept that the virus is present in the community (as long as it is within the baseline number), we live with it and take steps to identify, test, isolate and treat. Importantly, we don’t lockdown at a very low threshold.
“Mitigation” – moving forward
If we are to opt for “mitigation”, it is critical to ensure that we have sufficient resources to:
- Make testing affordable and available to all members of the community and without strict pre-testing criteria ( since the virus is already present in the community, the only criteria for testing should only be by “being in the community”);
- Conduct prevalence study to better titrate our “alert threshold for lockdown”;
- Conduct contact tracing for all sporadic cases timely (with the current 9,100 sporadic cases in Klang Valley, do we have enough health inspectors to conduct timeous and detailed contact tracing?);
- Admit to a hospital all individuals who have been tested positive – irrespective of asymptomatic, mild or severe cases;
- Take care of people's welfare during their period of quarantine/ lockdown.
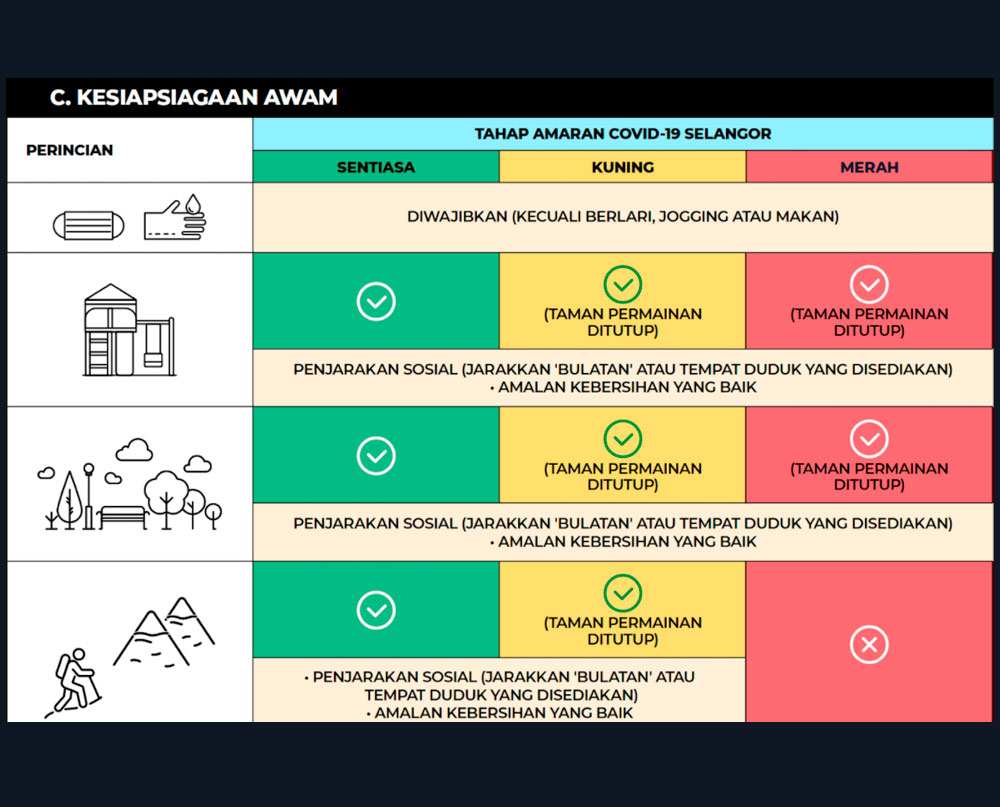
- Have better, more predicted, action guides for the community as opposed to ad-hoc standard operating procedures (SOPs). It will probably benefit everyone in order to plan their action when their area is reaching a certain threshold level (figure below enclosed as an example).
To ensure effective “mitigation”, neither MOH nor a central authority can do it alone. Other stakeholders need to be involved and consulted.
Additionally, it needs to mobilise local leaders, empower the community with transparent information and data and coordinate with state agencies.
Rethinking goals and realigning strategies
This is not a call to throw in the towel for the containment and control strategy. But this is a reality check to revisit our goals and to tune our strategy based on those goals. If we have no clear purpose, then it is hard to plan the strategy for it.
We cannot implement the same conditional MCO measure (with loose restriction and not investing in more resources in TTI ) and hope to achieve “containment” results similar to the post-MCO period. The last 14 days of conditional MCO does not seem to indicate that it is going to work.
Something must change.
Either we change our lockdown strategy to achieve “containment” - by opting for stricter measures, a more targeted area, and to also cover areas with sporadic cases too, and rapidly escalate our contact tracing personnel and capacity to outrace the transmission.
Otherwise, we must change our expectations and public health strategy to opt for “mitigation” – which require us to scientifically change our “alert threshold” and so there will not be a need to lock down Klang Valley for an arbitrary number of 40 positive cases.
DR HELMI ZAKARIAH is a public health and digital epidemiology enthusiast. - Mkini
The views expressed here are those of the author/contributor and do not necessarily represent the views of MMKtT.
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.