


Malaysia is currently faced with the third wave of Covid-19 cases and hence it is crucial that containment policies are informed by the latest scientific tools and innovations available.
This is to ensure that their policies are the best practices at hand, not just blunt and damaging tools such as lockdowns, but complementary tools, which are friendly to both lives and livelihoods, such as large-scale and frequent population-level testing strategy.
The recent upsurge of Covid-19 cases is much higher compared to the second wave in March. The magnitude of this third wave is so large that it would eclipse the total number of cases of the first wave in just hours. (see Diagram I).
Even more worrying is the increasing numbers of sporadic community cases not linked to a cluster. This makes contact tracing, quarantine and isolation much more challenging.
Challenges in containing Covid-19 will persist until we achieve herd immunity preferably through vaccination, the chances of which are higher as the science and technology minister has announced Malaysia’s participation, together with 172 countries, in the global Covax initiative.
RT-PCR is the gold standard for testing individuals for Covid-19 as it has very high analytical sensitivity and specificity. In simple terms, a high sensitivity means that almost all cases of Covid-19 will test positive and a high specificity means that almost all who test positive have Covid-19 (and not, for example, different coronavirus). However, as a public health tool applied at the population level, it has three critical drawbacks which preclude its large-scale use.
Firstly, it is costly and cumbersome. RT-PCR analysis requires a large laboratory, large investment costs of at least RM500,000, and substantial operating expenses. In the private sector, RT-PCR tests cost about RM400.
In Malaysia, the central laboratories are able to analyse 41,354 RT-PCR specimens per day. Laboratories in Sabah are already overwhelmed, prompting the defence minister to announce that the air force will ferry test specimens from Sabah to laboratories in Peninsular Malaysia.
Secondly, it takes a long time for test results to be available. Excluding the time required to transport specimens and notify patients, which would be substantial especially in the case of Sabah, an urgent RT-PCR specimen can be analysed in six hours but due to the backlog of tests, routine specimens take up to three to four days to be analysed. These few days are not just a source of anxiety for the individual tested, but represent lost livelihoods, delays in treatment, and delays in contact tracing.
Thirdly, as even minuscule amounts of viral genetic material can be detected, it does not differentiate highly infectious individuals (higher viral loads) from less infectious individuals with lower viral loads.
Enter antigen-based Covid-19 rapid test kits (RTK-Ag). As part of a population-level strategy to "sweep" and isolate infective individuals, RTKs have several appealing features.
Firstly, due to advances in technology, the tests are now exceedingly convenient. They can be performed at a longhouse ruai (hall) without equipment or electricity. RTKs can be stored at room temperature. Testing even in remote areas throughout the country would be as easy as in a central hospital.
Secondly, the tests are rapid. In the 15 minutes taken for a tested person to scroll through their WhatsApp messages, the tiny red line or lines that denote the test result will become available ala the consumer urine pregnancy tests that couples are familiar with.
Thirdly, it is cheap. Global institutions such as the World Health Organisation (WHO), with financial commitments from the Global Fund, are making 120 million affordable, quality RTKs available to the governments of countries without the need for a middle person. Malaysia is among the beneficiary countries.
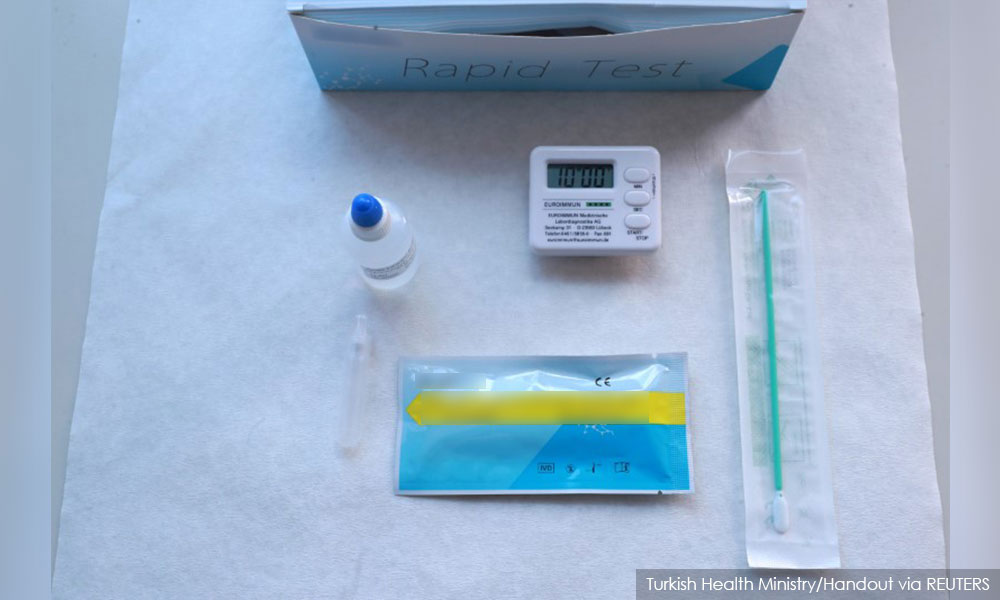
Each RTK-Ag is priced at a maximum of US$5 (RM20) – a typical household’s daily spend on food and perhaps not much different to the cost of food ratios supplied to those under enhanced movement control order (MCO). As this is point-of-care diagnostics, public health officials will also not need to spend time calling back the patient.
Fourthly, RTKs pick out infectious cases. In the context of a population-level strategy, the test can be better described as a test for Covid-19 infectivity rather than a test for Covid-19. This makes it a useful public health tool, different from RT-PCR. RT-PCR will remain a critical tool for the management of individual Covid-19 cases. Different tools for different purposes.
How could RTKs be used as part of a population-level strategy? In simple terms, to reduce Covid-19 infections we need to reduce four variables.
Firstly, the number of daily encounters between individuals – this is why lockdowns help, albeit at a cost to mental health and livelihoods.
Secondly, the chance that an encounter between individuals results in a spread of Covid-19 – this is why wearing masks, physical distancing, and washing hands help a lot.
Thirdly, the proportion of individuals who are susceptible to the disease – ie those who are not immune. This is why we await a Covid-19 vaccine with bated breath as there is no "exit" until herd immunity is reached, either by infection or preferably by vaccination.

Fourthly, the duration that individuals spend in an infective state within a community. This fourth variable can be reduced by a large-scale "sweep" and isolate strategy – by testing many people for infectivity often. Infective individuals can hence be quickly isolated from the rest of the community, limiting spread to others.
All these four variables work in tandem. Hence, to obtain a similar containment effect, if we do not wear face masks, a stronger lockdown would be needed, ceteris paribus.
Similarly, if most infective individuals can be quickly isolated from the community with large-scale and frequent testing with RTKs, we reduce our reliance on lockdowns, which harm mental health, prevent many from seeking healthcare for non-Covid-19 conditions, and devastate the economy.
In this critical third wave, Malaysia must use all the tools available at our disposal, not just lockdowns.
DR MUSA MOHD NORDIN is a paediatrician and chairperson of the Fima Advisory Council. - Mkini
The views expressed here are those of the author/contributor and do not necessarily represent the views of MMKtT.
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.